Bifogade filer
 File
File
Beskrivning
| Land | Storbritannien |
|---|---|
| Lista | FTSE 100 |
| Sektor | Hälsovård |
| Industri | Läkemedel & Handel |
Intresserad av bolagets nyckeltal?
Analysera bolaget i Börsdata!

Vem äger bolaget?
All ägardata du vill ha finns i Holdings!

Anselamimab demonstrated 62% improvement in survival and 71% reduction in cardiovascular hospitalisations in prespecified kappa light-chain amyloidosis subgroup. Results published in the Journal of Clinical Oncology and will be presented at 2026 American Society of Clinical Oncology Annual Meeting.
The global CARES Phase III clinical programme showed that treatment with anselamimab, a potential first-in-class anti-fibril therapy, resulted in nominally statistically significant and highly clinically meaningful benefit in adults with advanced kappa light chain (AL) amyloidosis as first-line therapy added to standard of care plasma cell dyscrasia (PCD) treatments, compared to placebo. In the overall population of patients with AL amyloidosis, treatment with anselamimab did not meet the primary endpoint, defined as a hierarchical combination of time to all-cause mortality (ACM) and frequency of cardiovascular hospitalisations (CVH), as previously disclosed.1
In a prespecified subgroup analysis of patients with kappa predominant light chain isotype, anselamimab improved survival by 62%, measured by ACM (hazard ratio 0.38; 95% confidence interval [CI] 0.17, 0.86; nominal p=0.012), and reduced the frequency of CVH by 71% (incidence risk ratio 0.29; 95% CI 0.10, 0.87; nominal p=0.028), compared to placebo in the subgroup with kappa AL amyloidosis.1
The reduction in the risk of ACM in the kappa subgroup was also observed in both trials comprising the CARES Phase III clinical programme among patients with kappa isotype with Mayo stage IIIa disease (75%) and Mayo stage IIIb disease (48%). No differences in ACM and CVH were observed among patients with lambda predominant light chain isotype.1
At 50 weeks, numerical improvements favoring anselamimab were observed in key secondary endpoints, including quality of life, as measured by the Kansas City Cardiomyopathy Questionnaire-Overall Score (Hodges-Lehmann median difference [HLMD]: 10.37 [95% CI -9.38, 25.56; p=0.113), and functional capacity, as measured by the Six-Minute Walk Test ([HLMD]: 18.00 [95% CI -71.60, 95.92; p=0.145), in patients with kappa light chain amyloidosis who received anselamimab, compared to placebo.1
AL amyloidosis is a rare, systemic and progressive disorder caused by defective plasma cells in the bone marrow. In AL amyloidosis, abnormal light chain proteins produced by these plasma cells misfold, aggregate and form amyloid fibrils that deposit in tissues and organs. Left untreated, the accumulation of these toxic amyloid deposits, particularly in the heart and kidneys, can cause progressive organ damage and dysfunction and may lead to premature death, most commonly due to cardiac failure.2-4 Worldwide, there are an estimated 74,000 patients living with AL amyloidosis, approximately 20% of whom have kappa light chain amyloidosis and approximately 80% of whom have lambda light chain amyloidosis.5-8
Ashutosh Wechalekar, FRCP, FRCPath, DM, Honorary Consultant Haematologist at University College London Hospitals and Professor of Medicine and Haematology at University College London, and lead principal investigator of the programme, said: "People living with advanced AL amyloidosis often face persistent, progressive and debilitating organ damage with no available options to target and clear existing amyloid fibril deposits. Results from the CARES Phase III programme show that anselamimab, a monoclonal antibody with a novel mechanism of action designed to target and remove amyloid fibrils, improved survival and reduced the frequency of cardiovascular hospitalisations in patients with kappa light chain amyloidosis. Anselamimab has the potential to offer a novel, clinically meaningful therapeutic for this subgroup of patients with kappa AL amyloidosis who can be easily identified by simple, routinely-used diagnostics."
Gianluca Pirozzi, Senior Vice President, Head of Development, Regulatory and Safety, Alexion, AstraZeneca Rare Disease, said: "The CARES Phase III programme is the first to show that targeting existing deposits of amyloid fibrils could deliver clinically meaningful survival and cardiovascular benefit in adults with kappa light chain amyloidosis, underscoring anselamimab's potential as a first-line therapy on top of standard of care. With anselamimab and our leading amyloidosis portfolio, we are advancing pioneering science with the goal of addressing critical treatment gaps. We look forward to continued engagement with health authorities to advance this potential first-in-class anti-fibril therapy."
Summary of hierarchical composite primary efficacy endpoint
Primary efficacy endpoints: overall population1
| Endpoint | Anselamimab (N = 271) | Placebo (N = 135) | P - Value | |
| ACM and CVH win ratio (95% CI) | 1.11 (0.83, 1.50) | 0.332 | ||
| ACM | n (%) | 90 (33.2) | 52 (38.5) |
|
| Hazard ratio (95% CI) | 0.80 (0.57, 1.13) | 0.290 | ||
| CVH | Frequency per year (95% CI) | 0.59 (0.42, 0.83) | 0.89 (0.55, 1.43) |
|
| Incidence risk ratio (95% CI) | 0.67 (0.39, 1.15) | 0.145 | ||
ACM, all-cause mortality; CVH, cardiovascular hospitalisation.
Primary endpoints: kappa and lambda isotype1
|
| Kappa isotype | Lambda isotype | |||||
| Endpoint | Anselamimab (N = 48) | Placebo (N = 24) | P - Value | Anselamimab (N = 219) | Placebo (N = 109) | P - Value | |
| ACM and CVH win ratio (95% CI) | 2.06 (0.98, 4.31) | 0.100 | 0.90 (0.64, 1.27) | 0.848 | |||
| ACM | n (%) | 15 (31.3) | 14 (58.3) |
| 73 (33.3) | 37 (33.9) |
|
| Hazard ratio (95% CI) | 0.38 (0.17, 0.86) | 0.012* |
1.02 (0.68, 1.52) | 0.647 | |||
| CVH | Frequency per year (95% CI) | 0.41 (0.20, 0.83) | 1.40 (0.58, 3.36) |
| 0.66 (0.44, 0.98) | 0.76 (0.43, 1.34) |
|
| Incidence risk ratio (95% CI) | 0.29 (0.10, 0.87) | 0.028* | 0.87 (0.46, 1.65) | 0.664 | |||
*Nominal statistical significance
ACM, all-cause mortality; CVH, cardiovascular hospitalisation.
All-cause mortality1
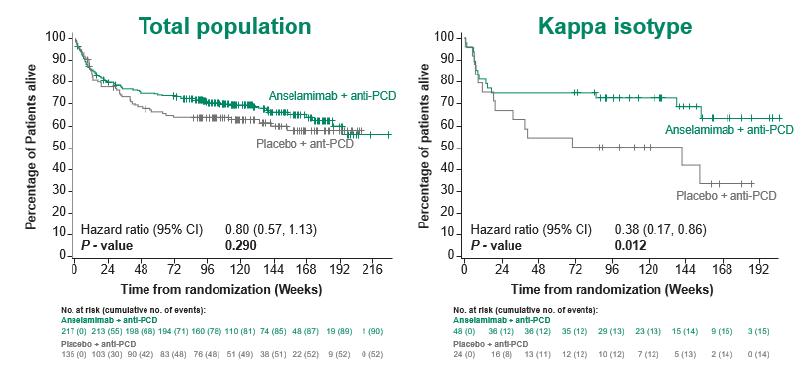
ACM, all-cause mortality; PCD, plasma cell dyscrasia.
Treatment with anselamimab was generally well tolerated in the overall population, including the kappa subgroup. Anselamimab had an acceptable safety profile, and the majority of adverse events were balanced between the anselamimab and placebo groups and consistent with the underlying medical condition and its treatment with standard of care plasma cell dyscrasia treatments.1
The results will be presented today at the 2026 American Society of Clinical Oncology (ASCO) Annual Meeting in Chicago, Illinois (Oral Abstract #7501) and published in the Journal of Clinical Oncology.1
Notes
Light Chain Amyloidosis
Light chain (AL) amyloidosis is a systemic and progressive type of amyloidosis where immunoglobulin light chain proteins, specifically kappa or lambda light chains, are produced abnormally by defective plasma cells in the bone marrow. These abnormal proteins misfold, aggregate and form amyloid fibrils that deposit and accumulate in tissues or organs, particularly in the heart and kidneys. The deposition can cause progressive damage and may lead to premature death, most commonly due to cardiac failure.2,3
In the early stages of the disease, people with AL amyloidosis may experience a range of vague signs and symptoms that mimic other diseases, which can often delay the diagnosis. Worldwide, there are an estimated 74,000 patients living with AL amyloidosis, approximately 20% of whom have kappa light chain amyloidosis and approximately 80% of whom have lambda light chain amyloidosis.5-8
CARES Phase III Clinical Programme
The Cardiac Amyloid Reaching for Extended Survival (CARES) clinical programme consists of two parallel global, Phase III, randomised, double-blind, placebo-controlled, multicentre trials evaluating the efficacy and safety of anselamimab plus standard of care (SoC) for underlying plasma cell dyscrasia in patients with light chain (AL) amyloidosis and cardiac involvement defined as European modification of Mayo 2004 stage IIIa and stage IIIb, respectively.9,10
The primary endpoint is a hierarchical combination of time to all-cause mortality (ACM) and frequency of cardiovascular hospitalisations (CVH) in the overall patient population across both trials. Key secondary endpoints include time to ACM and frequency of CVH analysed separately, functional capacity based on the Six-Minute Walk Test (6MWT), cardiac function using Global Longitudinal Strain (GLS%) and quality of life using the Kansas City Cardiomyopathy Questionnaire-Overall Score (KCCQ-QS).9,10
The CARES clinical programme is the largest prospective investigation in cardiac AL amyloidosis to date with a total of 406 patients enrolled from 19 countries globally, including 281 patients with stage IIIa and 125 patients with stage IIIb disease per European modification of the Mayo 2004 staging system.9,10
In CARES, newly diagnosed patients planning first-line plasma cell dyscrasia (PCD) treatment with cyclophosphamide, bortezomib and dexamethasone were randomised 2:1 to receive either anselamimab or placebo once weekly for the first four weeks and then every two weeks until study completion. Daratumumab was permitted but not required as part of the anti-PCD regimen. Approximately 80% of patients in CARES received daratumumab as part of their treatment.
Following the primary evaluation treatment period, which concluded 18 months after the last patient was randomised, all patients had the option to participate in an open-label extension period receiving anselamimab for up to 24 months, with or without anti-PCD treatment.9,10
Anselamimab
Anselamimab is an investigational, potential first-in-class anti-fibril therapy designed to improve organ function by reducing or depleting amyloid deposits in the tissues and organs of patients living with AL amyloidosis. By binding with specificity to targets within amino acids on misfolded amyloid fibrils, anselamimab promotes destruction and clearance of amyloid deposits, while sparing native free light chains from destruction. Anselamimab has been granted Fast Track Designation by the US Food and Drug Administration (FDA) and received Orphan Drug Designation from the US FDA, European Commission and the Ministry of Health, Labour and Welfare of Japan for the treatment of AL amyloidosis.
Alexion
Alexion, AstraZeneca Rare Disease, is focused on serving patients and families affected by rare diseases and devastating conditions through the discovery, development and delivery of life-changing medicines. A pioneering leader in rare disease for more than three decades, Alexion was the first to translate the complex biology of the complement system into transformative medicines, and today it continues to build a diversified pipeline across disease areas with significant unmet need, using an array of innovative modalities. As part of AstraZeneca, Alexion is continually expanding its global geographic footprint to serve more rare disease patients around the world. It is headquartered in Boston, US.
AstraZeneca (LSE/STO/NYSE: AZN) is a global, science-led biopharmaceutical company that focuses on the discovery, development, and commercialisation of prescription medicines in Oncology, Rare Disease, and BioPharmaceuticals, including Cardiovascular, Renal & Metabolism, and Respiratory & Immunology. Based in Cambridge, UK, AstraZeneca's innovative medicines are sold in more than 125 countries and used by millions of patients worldwide. Please visit astrazeneca.com and follow the Company on Social Media @AstraZeneca.
Contacts
For details on how to contact the Investor Relations Team, please click here. For Media contacts, click here.
References
- Wechalekar A, et al. Phase 3 randomized trial to evaluate the impact of anselamimab on all-cause mortality in κ light-chain amyloidosis. Presented at the American Society of Oncology (ASCO) Annual Meeting; 2026 May 29; Chicago, IL.
- Desport E, et al. AL amyloidosis. Orphanet J Rare Dis. 2012;7(54).
- Grogan M, et al. Light-chain cardiac amyloidosis: strategies to promote early diagnosis and cardiac response. Heart. 2017;103(14):1065-1072.
- Mollee P, et al. How to diagnose amyloidosis. Internal Medicine Journal. 2014;44:7-17.
- Wechalekar AD, et al. AL amyloidosis for cardiologists; awareness, diagnosis, and future prospects. JACC: CardioOncol. 2022;4(4):427-441.
- Kumar N, et al. Global epidemiology of amyloid light-chain amyloidosis. Orphanet J Rare Dis. 2022;17(1):278.
- Merlini G. AL amyloidosis: from molecular mechanisms to targeted therapies. Hematology Am Soc Hematol Educ Program. 2017;2017(1):1-12.
- Manwani R, et al. A prospective observational study of 915 patients with systemic AL amyloidosis treated with upfront bortezomib. Blood. 2019;134(25):2271-2280.
- ClinicalTrials.gov. A study to evaluate the efficacy and safety of CAEL-101 in patients With Mayo Stage IIIa AL amyloidosis (CARES). NCT Identifier: NCT04512235. Available here. Accessed May 2026.
- ClinicalTrials.gov. A study to evaluate the efficacy and safety of CAEL-101 in patients with Mayo Stage IIIb AL amyloidosis (CARES). NCT Identifier: NCT04504825. Available here. Accessed May 2026.